About SBHI
Strategic Behavioral Health Initiative
The Strategic Behavioral Health Initiative (SBHI) aims to assess current behavioral health needs and resources for children and youth and develop a roadmap to a comprehensive continuum of care that meets the needs of children and youth throughout San Diego County.



There is a mental health crisis among children and youth that has only worsened with the COVID-19 pandemic. The Strategic Behavioral Health Initiative will
convene community stakeholders, including parents and youth, healthcare providers, early care & education, the County of San Diego, and community-based
organizations. Convenings and collaboration will result in a more complete understanding of the pediatric behavioral health ecosystem, resources, and best practices for children and youth. Findings will be used to leverage additional behavioral health resources and identify a reimagined behavioral health system of care for children and youth in San Diego County.
CALL TO ACTION
The Strategic Behavioral Health Initiative (SBHI) aims to assess current behavioral health needs and resources for children and youth in San Diego County and develop a roadmap to a comprehensive continuum of care.
TARGET POPULATION
Children and youth in San Diego County.
ESTABLISHED
July 2023
INITIAL AREAS OF FOCUS:
-
Promotion & Prevention
-
Care Coordination & Integration
-
Clinical Pathways
-
System & Payment Reform
-
Workforce Development
Funders

AAP-CA3'S ROLE
- Map existing child & youth behavioral health services & programs.
- Identify local and national best practices.
- Complete state & federal policy scan of existing & future funding opportunities & relevant policies.
- Convene & support the steering committee, advisory committee, & working groups.
- Create an advocacy plan and roadmap.
ABOUT AAP-CA3
Steering Committee:
Name | Orginazation | Speciality |
|---|---|---|
Moises Baron, PhD | Former CEO, San Diego Center for Children | Specialty Mental Health |
Luke Bergman, PhD | Director, County of San Diego Behavioral Health Services | County Behavioral Health |
David Bond, LCSW | Director of Behavioral Health Enterprise and Government Affairs, Blue Shield Promise | Medi-Cal Health Plan |
Karen Connolly | Senior Director of Workforce Development, San Diego Regional Policy Innovation Center | Workforce |
Michelle Dern, MD | Pediatrician, Scripps Coastal Medical Center | Pediatrician |
Pradeep Gidwani, MD | Medical Director, AAP-CA3 | Early Childhood |
Ben Maxwell, MD | Division Chief of Child & Adolescent Psychiatry, Rady Children’s Hospital San Diego | Hospital |
Heather Nemour | Coordinator Student Support Services and Programs Division, San Diego County Office of Education | Schools |
Jeff Rowe, MD | Child Psychiatrist | Psychiatrist |
Marisa Varond | Executive Director, McAlister Institute | Executive Director, McAlister Institute |
Aimee Zeitz | Executive Director of Community Wellbeing, YMCA of San Diego County | Early Care and Education |
Continuum of Care:
Population:
Problem and Need Data Resources:
AAP-AACAP-CHA Declaration of a National Emergency in Child and Adolescent Mental Health (2021): AAP-AACAP-CHA Declaration of a National Emergency in Child and Adolescent Mental Health
Rates of childhood mental health concerns and suicide rose steadily between 2010 and 2020 and by 2018 suicide was the second leading cause of death for youth ages 10-24. The pandemic has intensified this crisis: across the country we have witnessed dramatic increases in Emergency Department visits for all mental health emergencies including suspected suicide attempts.
US Surgeon General’s Advisory – Protecting Youth Mental Health (2021): surgeon-general-youth-mental-health-advisory.pdf (hhs.gov)
The U.S. surgeon general issued an Advisory on Protecting Youth Mental Health, which outlines the pandemic’s unprecedented impacts on the mental health of America’s youth and families and the mental health challenges that existed long before the pandemic.
- It is estimated that as of June 2021, more than 140,000 children in the U.S. had lost a parent or grandparent caregiver to COVID-19.
- In 2019, before the pandemic, one in three high school students and half of the female students reported persistent feelings of sadness or hopelessness, an overall increase of 40% from 2009.
- Socioeconomically disadvantaged children and adolescents — for instance, those growing up in poverty — are two to three times more likely to develop mental health conditions than peers with higher socioeconomic status.
US Surgeon General’s Advisory – Social Media and Youth Mental Health (2023): Social Media and Youth Mental Health (hhs.gov)
- Up to 95% of youth ages 13–17 report using a social media platform, with more than a third saying they use social media “almost constantly.”
- Adolescent social media use is predictive of a subsequent decrease in life satisfaction for certain developmental stages including for girls 11–13 years old and boys 14–15 years old.
- A longitudinal cohort study of U.S. adolescents aged 12–15 (n=6,595) that adjusted for baseline mental health status found that adolescents who spent more than 3 hours per day on social media faced double the risk of experiencing poor mental health outcomes including symptoms of depression and anxiety.
Kaiser Family Foundation: Recent Trends in Mental Health and Substance Abuse Concerns Among Adolescents (Published February 3, 2024): Recent Trends in Mental Health and Substance Use Concerns Among Adolescents | KFF
Key takeaways include:
- In 2021 and 2022, 21% of adolescents reported experiencing symptoms of anxiety in the past two weeks and 17% reported experiencing symptoms of depression. Female and LGBT+ adolescents were more likely than their counterparts to report experiencing anxiety or depression.
- Deaths due to drug overdose among adolescents more than doubled from 2018 (253 deaths) to 2022 (723 deaths). The largest increases in these deaths were among Hispanic and Black adolescents.
- Suicides are the second leading cause of death among adolescents. These deaths peaked in 2018 but have declined in recent years. In 2022, suicide death rates were highest among American Indian and Alaska Native adolescents (22.2 per 100,000) followed by White adolescents (7.2 per 100,000). Adolescent males had higher rates of suicide compared to their female peers (8.1 vs. 3.8 per 100,000) in 2022; however, thoughts of suicide and suicide attempts were higher (and increased faster) for females.
- In 2021 and 2022, 20% of adolescents reported receiving mental health therapy and 14% reported taking prescription medication. In general, LGBT+ and female adolescents were more likely to report receiving treatment than their counterparts.
- Many adolescents reported adverse experiences, including bullying (34%), emotional abuse by a parent (17%), and neighborhood violence (15%) in 2021 and 2022. Ninety-two percent of adolescents reported extended use of screens, which can also negatively impact mental health and well-being.
CDC National Health Interview Survey Teen – Interactive Summary Health Statistics for Teens (Published 2023): NHIS Teen (cdc.gov)
Grade – Supporting Mental Health: D+
Grade – Preventing Substance Abuse: D-
The Department of Health Care Services (DHCS) and the Department of Managed Health Care (Managed Health Care) can do more to detect and address challenges that children in Medi‑Cal face when seeking behavioral health services. Behavioral health care includes care for both mental health and substance use issues, and research indicates that timely access to this care is critical. State law provides that timely access is the allowable time frame by which a health care service plan must offer appointments to members. Though there are no statewide data to demonstrate precisely how long it takes Medi‑Cal patients to receive behavioral health care once they request it, survey data for appointment wait times show that many Medi‑Cal managed care plans are unable to provide timely access for children. For example, 43 percent of urgent appointments with psychiatrists DHCS surveyed in 2022 exceeded the 96‑hour appointment wait time standard, and the median wait time for those appointments was almost 13 days.
The Annie E. Casey Foundation 2022 Kids County Data Book – State Trends in Child Well-Being (2022.)
Each year, the Data Book tracks how children are faring nationally and in every state through indicators in the areas of economic well-being, education, health and family and community. Many of these affect or are themselves affected by children’s and families’ mental health. In California, the percentage of children (ages 2-17) who had anxiety or depression increased by 70%.
The HASD&IC Needs Assessment provides community input survey information, contributing factors to youth behavioral health needs, and critical deficits across the continuum (of care,) which include:
- Increased Emergency Department Volume
- Family Support and Respite Care
- Emergency Shelter
- Workforce Shortage
This report summarizes cumulative system demographics and clinical outcomes for children and adolescents served by the County of San Diego’s, Health and Human Services Agency (HHSA), Children, Youth & Families Behavioral Health Services (CYFBHS) in Fiscal Year (FY) 2021-22 (July 2021 – June 2022). CYFBHS System of Care serves children and youth up to age 21, as well as a perinatal population. The primary focus of this annual report is CYFBHS mental health services, with limited information also available on prevention, early intervention, and addiction treatment.

When the data from all 192 studies were integrated, the authors found that the peak age of onset for mental disorders was 14.5 years. About 34.6 percent of patients showed a disorder before the age of 14, 48.4 percent before the age of 18, and 62.5 percent before the age of 25 years. This shows that for almost 50 percent of patients, mental disorders start before they reach adulthood, highlighting the importance of early intervention and prevention measures for mental health issues in adolescents.
Roadmaps and Guidelines:

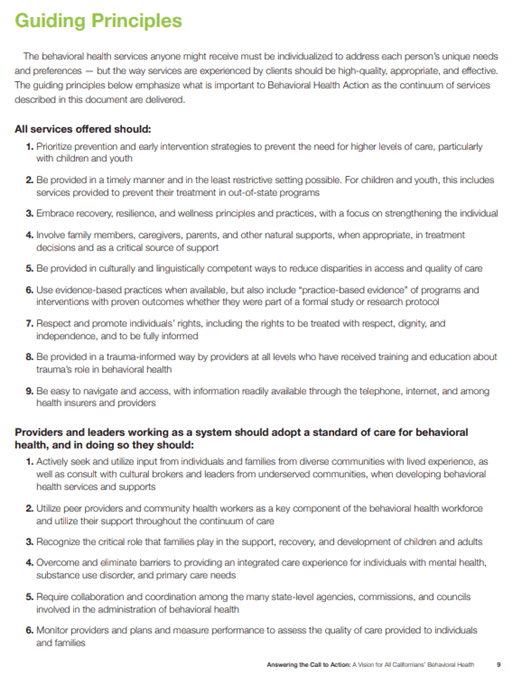
CONCLUSION: Over time, this plan will lead California to a behavioral health system that:
- Reduces misinformation, stigma and discrimination and increases knowledge, acceptance and support for care;
- Reduces the delay from the onset of symptoms to treatment and increases ongoing engagement in care;
- Reduces disparities in utilizing services among BIPOC and LGBTQ+ communities and increases access to culturally responsive care;
- Reduces the proportion of individuals with mental health and substance use disorders in prisons and jail and increases high-quality community care placements;
- Reduces the risk of homelessness and housing insecurity and increases educational and employment opportunities; and
- Reduces disappointment and frustration and increases satisfaction and trust in the quality of services received.
Health Equity in Access to Behavioral Health Recovery Services (HEAR US) is a special statewide project funded by the California Department of Health Care Services (DHCS) and managed by The Center at Sierra Health Foundation (The Center). The overarching goal of HEAR US is to increase the number and quality of culturally responsive behavioral health recovery services and programs tailored to local needs in California. The project focuses on promoting accessible and equitable behavioral health care for people with serious mental illness (SMI), serious emotional disturbance (SED), and substance use disorder (SUD). An additional focus is on improving this care for underserved populations, including Black, Indigenous, Latine, Asian Pacific Islander, people with disabilities, and 2S/LGBTQ+ communities.

National Academies of Sciences, Engineering and Medicine. Fostering Healthy Mental, Emotional, and Behavioral Development in Children and Youth: A National Agenda (2019)
National Academies of Sciences, Engineering and Medicine (Committee on Fostering Healthy Mental, Emotional, and Behavioral Development Among Children and Youth; Board on Children, Youth, and Families; Division of Behavioral and Social Sciences and Education.) Fostering Healthy Mental, Emotional, and Behavioral Development in Children and Youth: A National Agenda. (2019)
FIGURE 11-1Interventions across the life course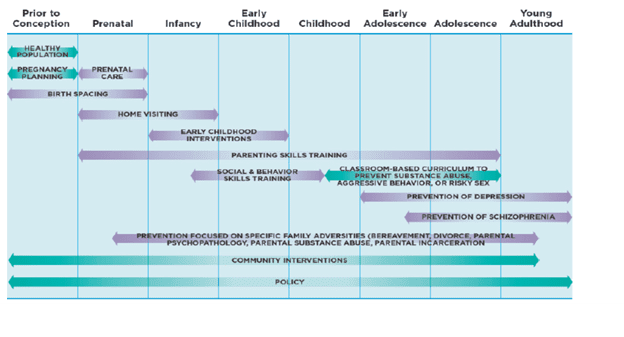
“First and foremost, this document was written in response to the overwhelming need in the County of San Diego for an integrated and effective response to individuals struggling with serious mental illness. The research was designed to provide insight to hospital CEOs, County healthcare providers, and other healthcare systems and entities who care for these vulnerable individuals. This paper shares the many challenges and opportunities identified by organizations, individual providers, and experts who encounter this population daily.
The bulk of information gathered and presented in this report derives from feedback regarding adult behavioral health treatment issues; however, SED children’s needs are equally important and the underlying system limitations are much the same. Although some issues and perspectives regarding children’s behavioral health were discussed in interviews and included in this summary report, a much more comprehensive analysis including additional pediatric clinicians, schools, and other children’s service providers is merited.”
This report outlines five recommendations that together make up a regional strategy designed to attract and retain the most resilient, representative, skilled and qualified behavioral health workforce in the United States. While these recommendations are presented in separate subsections, they are parts of a single vision. If implemented in isolation, they will have less than desired results.
- Invest in competitive compensation
- Pursue administrative relief opportunities
- Establish regional training hubs
- Build a regional workforce training fund
- Continue listening to workers ASPE Issue Brief: HHS Roadmap for Behavioral Health Integration (Published September 2022): HHS Assistant Secretary for Planning and Evaluation (ASPE,) Issue Brief: HHS Roadmap for Behavioral Health Integration (September 2022.)
KEY POINTS:
- HHS is committed to providing the full spectrum of integrated, equitable, evidence-based, culturally appropriate, and person-centered behavioral health care to the populations it serves.
- HHS has evaluated key barriers to transforming behavioral health care in line with President Biden’s Strategy to Address our National Mental Health Crisis and has identified policy solutions to overcome these barriers.
- HHS will advance the Strengthen System Capacity pillar in the President’s national strategy by developing a diverse workforce prepared to practice in integrated settings and investing in infrastructure for integrated care.
- HHS will advance the Connect Americans to Care pillar by leveraging health financing arrangements, including efforts to fully realize the potential of parity.
- HHS will advance the Support Americans by Creating Healthy Environments pillar through investments in behavioral health promotion, upstream prevention, and recovery.

State:
1. BH-CONNECT – Section 1115 demonstration
2b. Evidence -Based Practices and/or Community Defined Evidence Practices (EBP/CDEP) Grant Program
3. Medi-Cal Transformation (previously known as Cal-AIM)
5. Governor Newsome Behavioral Health Reform: Prop 1 – March 2024 Ballot
State:
1. Medi-Cal (CalAIM) Section 1115 Waiver
On October 20, 2023, the Department of Health Care Services (DHCS) today submitted to the Centers for Medicare & Medicaid Services (CMS) a proposed amendment to the California Advancing and Innovating Medi-Cal (CalAIM) Section 1115 demonstration related to transitional rent services and the new Section 1115 demonstration request, entitled the California Behavioral Health Community-Based Organized Networks of Equitable Care and Treatment (BH-CONNECT) demonstration.
The BH-CONNECT demonstration builds upon unprecedented investments and policy transformations currently underway in California that are designed to expand access to community-based behavioral health care and improve outcomes for Medi-Cal members living with the most significant mental health and substance use needs. California has invested more than $10 billion and is implementing landmark policy reforms to strengthen the behavioral health care continuum through initiatives like the Children and Youth Behavioral Health Initiative, Behavioral Health Continuum Infrastructure Program, Behavioral Health Bridge Housing Program, CalAIM Justice-Involved Initiative, Behavioral Health Payment Reform, mobile crisis and 988 expansion, and more.
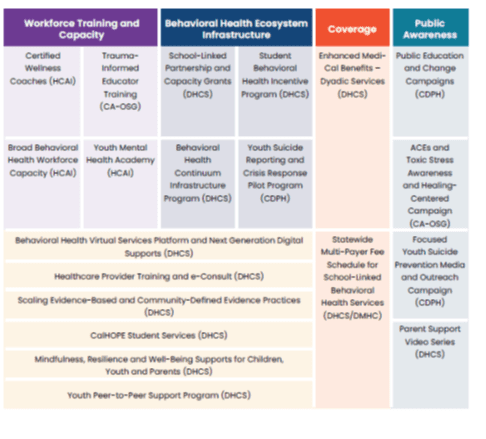
2. CYBHI
Established as part of the Budget Act of 2021, the CYBHI is a multiyear, multi-department package of investments that seeks to reimagine the systems, regardless of payer, that support behavioral health for all California’s children, youth, and their families. Efforts will focus on promoting social and emotional well-being, preventing behavioral health challenges, and providing equitable, appropriate, timely, and accessible services for emerging and existing behavioral health (mental health and substance use) needs for children and youth ages 0-25.
The DHCS is responsible for key work streams under this initiative, including but not limited to:
- Development a Behavioral Health Virtual Services & E-consult Platform;
- Development of a Statewide Multi-Payer School-linked Fee Schedule and Behavioral Health Provider Network;
- Issuance of Grants to Scale Evidence-Based Practices and Community-Defined Evidence Practices;
- Issuance of School-Linked Partnership and Capacity Grants;
- Implementation of Dyadic Services as a Medi-Cal Benefit;
- Development of Parent Support Video Series;
- Issuance of Youth Peer-to-Peer Support Programs;
- Development of CalHOPE Student Support;
- Issuance of Mindfulness, Resilience, and Wellbeing Supports;
- Development of Next Generation Digital Technologies; and,
- Development of a Behavioral Health Continuum Infrastructure Program.
The Department of Health Care Services (DHCS) will implement the Student Behavioral Health Incentive Program (SBHIP), which seeks to address behavioral health access barriers for Medi-Cal students through Targeted Interventions that increase access to preventive, early intervention, or other behavioral health services provided by school-affiliated behavioral health providers for TK-12 children in public schools.
The SBHIP program is implemented in phases. Calendar Year (CY) 2022 primarily focused on building relationships between local educational agencies and Medi-Cal managed care plans (MCPs) to develop a behavioral health needs assessment of the local student population. In addition, MCPs and their local partners selected Targeted Interventions and submitted project plans to DHCS. Upon DHCS approval of the project plans, the MCPs and local partners began implementing Targeted Interventions in selected schools. CY 2023 and 2024 will focus on implementing and sustaining the chosen interventions.
2b. Issuance of Grants to Scale Evidence-Based Practices and Community-Defined Evidence Practices
The Department of Health Care Services (DHCS) will distribute grants to organizations seeking to scale evidence-based and/or community-defined evidence practices (EBPs/ CDEPs) that improve youth behavioral health based on robust evidence for effectiveness, impact on racial equity, and sustainability. By scaling EBPs and CDEPs throughout the state, DHCS aims to improve access to critical behavioral health interventions, including those focused on prevention, early intervention, and resiliency/recovery for children and youth, with a specific focus on children and youth who are from either or both of the following groups: Black, Indigenous, and People of Color (BIPOC) and the LGBTQIA+ community.
Through six competitive grant funding rounds, DHCS will award grants, totaling approximately $429 million, in the following focus areas:
- Round 1: Parent/caregiver support programs and practices
- Round 2: Trauma-informed programs and practices
- Round 3: Early childhood wraparound services
- Round 4: Youth-driven programs
- Round 5: Early intervention programs and practices
- Round 6: Community-defined programs and practices
2c. Dyadic Benefit
- Per California Welfare and Institutions Code section 14132.755, the Dyadic Services benefit is a family- and caregiver-focused model of care intended to address developmental and behavioral health conditions of children as soon as they are identified, and that fosters access to preventive care for children, rates of immunization completion, coordination of care, child social-emotional health and safety, developmentally appropriate parenting, and maternal mental health.1 The dyadic services benefit is designed to support implementation of comprehensive models of dyadic care, such as Healthy Steps and Dulce, that work within the pediatric clinic setting to identify and address caregiver and family risk factors for the benefit of the child.

3. Medi-Cal Transformation / Cal-AIM
The Department of Health Care Services (DHCS) has developed a framework that encompasses broad-based delivery system, program and payment reform across the Medi-Cal program, called CalAIM: California Advancing and Innovating Medi-Cal. CalAIM advances several key priorities of the Administration by leveraging Medicaid as a tool to help address many of the complex challenges facing California’s most vulnerable residents, such as homelessness, behavioral health care access, children with complex medical conditions, the growing number of justice involved populations who have significant clinical needs, and the growing aging population.
To achieve such principles, CalAIM has three primary goals:
- Identify and manage member risk and need through whole person care approaches and addressing Social Determinants of Health;
- Move Medi-Cal to a more consistent and seamless system by reducing complexity and increasing flexibility; and
- Improve quality outcomes, reduce health disparities, and drive delivery system transformation and innovation through value-based initiatives, modernization of systems and payment reform.
3a. Enhanced Care Management and Community Supports:
California is transforming Medi-Cal to provide members with more comprehensive, coordinated, person-centered, and equitable care. Enhanced Care Management (ECM) and Community Supports are two major new Medi-Cal programs that launched in 2022 and serve a growing number of Californians. ECM is a comprehensive care management benefit to address clinical and non-clinical needs for the highest-need members enrolled in Medi- Cal managed care plans (MCPs).
4. Workforce
State: California Department of Health Care Access and Information Workforce Initiatives
Local: On October 11, 2022, The County Board of Supervisors received the report titled, “Addressing San Diego’s Behavioral Health Workforce Shortage” and directed the CAO to report back. The report outlined five recommendations to address San Diego’s workforce shortage:
- Invest in competitive compensation;
- Pursue administrative relief;
- Build regional workforce training fund;
- Establish regional training centers of excellence; and
- Continue listening to workers.
5. Governor Newsome Behavioral Health Reform: Prop 1 – March 2024 Ballot:
Proposition 1
Proposition 1 has two major components related to providing mental health care and drug or alcohol treatment to people and addressing homelessness. The proposition:
- Changes the Mental Health Services Act that was passed by voters in 2004, with a focus on how the money from the act can be used.
- Approves a $6.4 billion bond to build (1) more places for mental health care and drug or alcohol treatment and (2) more housing for people with mental health, drug, or alcohol challenges.
The legislative package, SB 326 & AB 531, focuses on five solutions to transform California’s behavioral health system through housing with accountability and reform with results:
- Reforming the Mental Health Services Act to provide services to the most seriously ill and to treat substance use disorders
- Building a workforce to reflect and connect with California’s diversity
- Focusing on outcomes, accountability, and equity
- Housing and behavioral health treatment in unlocked, community-based settings
- Housing for veterans with behavioral health challenges



Interdisciplinary, team-based pediatric integrated mental healthcare has been shown to be efficacious, accessible, and cost-effective. Measurement-based care has been implemented and preliminary results indicate that patient response to therapy has resulted in a 44% reduction in anxiety symptoms and a 62% decrease in depression symptoms.
Content